The concept of intranasal peptide delivery blood-brain barrier research has quietly reshaped how scientists think about central nervous system access. For decades, the blood-brain barrier stood as the defining obstacle in neurological and cognitive research: a selective filtration system so effective that the vast majority of therapeutic compounds never reach brain tissue in meaningful concentrations. Intranasal administration offers a structurally different route, one that bypasses the barrier rather than attempting to cross it. The olfactory and trigeminal nerve pathways that run from the nasal epithelium directly into the cranial vault have attracted serious scientific attention, and the peptide research emerging from this field is considerable.
This isn't speculative territory anymore. Published work in neuropharmacology and delivery science has documented the transport of intact peptide molecules along axonal and perineural channels, suggesting that molecular size and lipophilicity constraints that typically govern blood-brain barrier penetration become less relevant when the nasal route is used. That has significant implications for a range of research areas, from neuroprotective peptide studies to investigations into cognitive performance, neuroinflammation, and sleep architecture.
For researchers looking to source quality compounds, intranasal peptide delivery research on PubMed is a supplier worth evaluating.
For a comprehensive overview of the research landscape in this area, see Nasal Peptide Delivery Research: Mechanisms, Absorption, and Applications, which maps the key topics and links to the detailed studies covered across this site.
The blood-brain barrier is a product of specialized endothelial cells lining cerebral capillaries, reinforced by tight junction proteins, astrocytic end-feet, and efflux transporters like P-glycoprotein. This architecture evolved to protect the brain from pathogens, toxins, and immune activity that would be damaging to neuronal tissue. It does its job well. Most small molecules that don't meet a narrow set of physicochemical criteria, primarily low molecular weight and high lipid solubility, are either excluded outright or actively pumped back out.
Peptides are structurally complex, often hydrophilic, and metabolically fragile. They face enzymatic degradation in the gastrointestinal tract, rapid hepatic clearance if they reach systemic circulation, and then the barrier itself if they manage all of that. Research on systemic peptide bioavailability consistently documents these compounding inefficiencies. This is exactly why nasal delivery has attracted such attention as an alternative pathway. The route doesn't require systemic exposure to achieve central access, at least in principle.
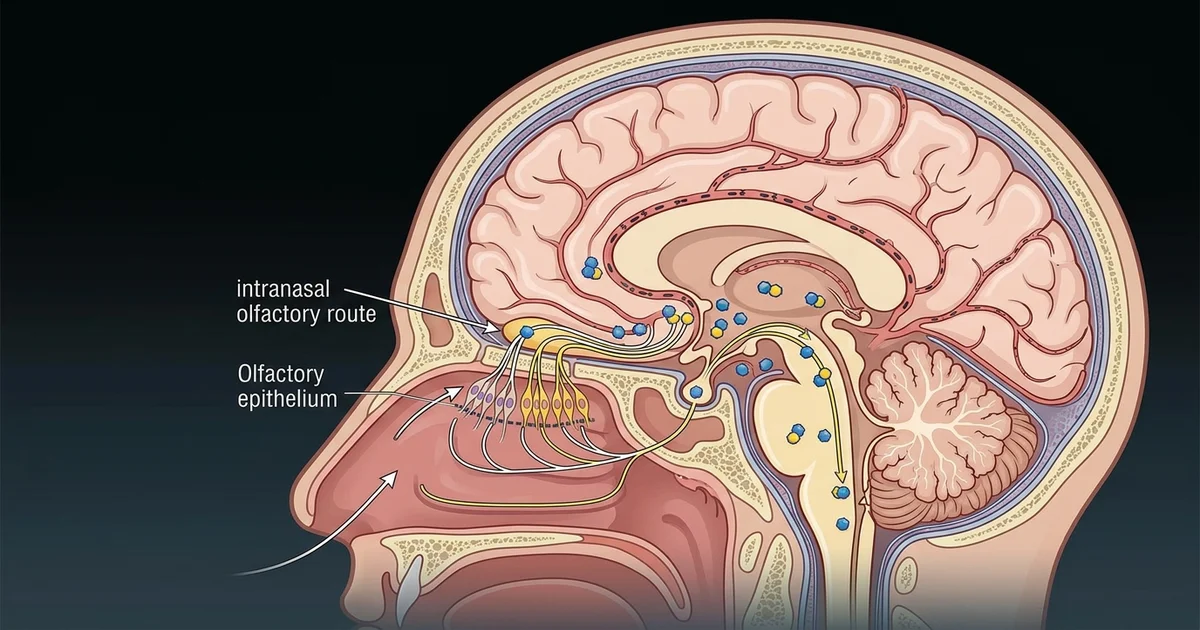
The nasal epithelium is thin and highly vascularized, which does support some systemic absorption. But the more scientifically interesting pathway runs through the olfactory submucosa, where nerve fibers from cranial nerve I pass through the cribriform plate and connect to the olfactory bulb. This is essentially a structural bridge between the outside world and the CNS. The trigeminal nerve adds a parallel pathway, particularly relevant for the brainstem and deeper structures. Together, these routes provide access that doesn't involve capillary crossing at all.
There are at least three proposed mechanisms by which intranasally applied compounds travel to brain tissue. Transcellular transport involves compounds passing through olfactory sensory neurons. Paracellular transport moves substances through spaces between epithelial cells. Perineural transport travels along the outer sheaths of nerve bundles, carried partly by bulk flow of interstitial fluid. Research suggests that peptides with certain structural characteristics preferentially use one pathway over another, though the precise determinants are still being worked out.
Transport isn't instantaneous. Pharmacokinetic studies using labeled compounds in animal models have detected uptake in the olfactory bulb within minutes of nasal application, but distribution to more distal regions like the hippocampus or prefrontal cortex takes longer and may involve secondary transport mechanisms. The trigeminal pathway appears to contribute to brainstem concentrations specifically, which has relevance for researchers studying autonomic function and sleep regulation.
Formulation matters considerably. The nasal mucosa presents its own enzymatic environment, and mucociliary clearance is a real constraint: the cilia lining the nasal passage continuously move mucus and its contents toward the nasopharynx, where it's swallowed. Compounds that aren't absorbed or transported quickly get cleared. Research into excipients, mucoadhesive agents, and nanoparticle carriers has grown substantially as a result. Cyclodextrins, chitosan-based gels, and lipid nanoparticles are among the delivery vehicles that have been studied for enhancing peptide stability and residence time at the epithelial surface.
Several classes of peptide have appeared in preclinical and clinical nasal delivery research. Insulin is perhaps the most extensively studied, given its documented effects on hippocampal function and insulin signaling in the brain independent of its peripheral metabolic role. Intranasal insulin trials in humans have examined effects on memory consolidation, which connects this work to broader interest in cognitive performance optimization, a subject with its own growing research literature.
Oxytocin administered intranasally is another well-documented example. Research suggests that nasally delivered oxytocin reaches cerebrospinal fluid at concentrations higher than would be predicted from systemic absorption alone, lending indirect support to the nose-to-brain transport hypothesis. The behavioral and social cognition effects observed in oxytocin research have made it a reference compound for delivery scientists trying to validate the pathway.
Neuroprotective peptides represent a particularly active research area. Compounds studied in the context of neuroinflammation, oxidative stress, and neuronal repair have been formulated for nasal delivery specifically because their CNS targets would be inaccessible by conventional systemic routes. Some of these peptides share structural or functional territory with compounds studied in broader peptide research, including work on tissue repair peptides and their potential effects on systemic and localized healing processes. The mechanistic overlap between peripheral and central peptide action is a recurring theme in the literature.
Growth hormone-releasing peptides and their analogs have also appeared in CNS delivery contexts. Research into ghrelin and ghrelin mimetics, for instance, has examined central effects on appetite regulation, energy balance, and sleep architecture, areas that overlap with interest in recovery optimization and hormonal peptide research more broadly.
The theoretical elegance of nasal delivery doesn't fully translate into simple practice. Nasal anatomy varies substantially between individuals, and conditions like mucosal congestion, septum deviations, or atrophic rhinitis can meaningfully alter delivery outcomes. The absorptive surface area in humans is smaller than in the rodent models where much of the foundational work has been conducted, which creates scaling challenges that aren't trivial to solve.
Delivery devices introduce another variable. Drops, sprays, and powder insufflation systems deposit compounds in different regions of the nasal cavity, and not all regions are equal for CNS transport. The olfactory epithelium is located in the upper posterior nasal cavity, an area that standard spray devices often don't reliably reach. Specialized devices designed to direct flow to the olfactory region have been developed, and research suggests that targeted deposition meaningfully improves CNS uptake efficiency compared to conventional nasal sprays.
Peptide stability during formulation and storage adds another layer. Many peptides are sensitive to pH, temperature, and oxidative conditions. Preservatives used in nasal formulations can interact with peptide structure. These aren't insurmountable obstacles, but they require careful formulation science and represent real limitations in current practice.
One acknowledged limitation worth naming directly: the evidence base for nose-to-brain peptide transport in humans remains thinner than the preclinical literature suggests it should be. Animal model findings, particularly in rodents, don't always replicate cleanly in human subjects, and the clinical trials that have been conducted on intranasal peptide delivery are often limited by small sample sizes and heterogeneous methodologies. The field is productive, but definitive clinical validation for many specific peptide compounds is still pending.
The practical draw of intranasal delivery for researchers focused on cognition and neuroprotection is straightforward: compounds that might influence neuroplasticity, synaptic signaling, or neuroinflammatory pathways can potentially be studied with CNS targeting that doesn't require invasive administration. This has implications for research on brain-derived neurotrophic factor analogs, which are large molecules that face significant barrier challenges via systemic routes. It also connects to research interest in peptides that interact with the hypothalamic-pituitary axis, given that nasal delivery could reach hypothalamic nuclei via olfactory tract projections.
Sleep regulation research has taken particular interest in the trigeminal pathway. Peptides with putative effects on sleep architecture, including some studied in the context of recovery and circadian rhythm optimization, have been formulated for nasal delivery precisely because brainstem nuclei involved in sleep-wake cycling are accessible via the trigeminal route. The connection between peptide research focused on sleep, recovery optimization, and nasal delivery science is a natural one.
Neuroinflammation is another convergence point. Research on peptides with anti-inflammatory properties has examined whether central neuroinflammatory pathways, increasingly implicated in mood disorders and cognitive decline, can be reached without the systemic exposure that might accompany injectable or oral administration. Whether intranasal delivery offers a practical solution here remains an active question, not a settled one.
The blood-brain barrier will remain a central problem in neuropharmacology and CNS-focused research. The nose-to-brain pathway represents a structurally legitimate, scientifically documented alternative route, not a workaround built on wishful thinking. The peptide research emerging in this space is worth tracking closely, particularly as formulation science matures and clinical evidence accumulates.
This article is for informational and research purposes only. Nothing in this article constitutes medical advice, a treatment recommendation, or guidance on clinical use of any compound. The information presented here is intended for educational and research discussion only. Consult a qualified healthcare professional before making any decisions related to health, supplementation, or therapeutic interventions. For research purposes only — not medical advice.