This article is for informational and research purposes only. The content does not constitute medical advice, diagnosis, or treatment recommendations. Always consult a qualified healthcare professional before making decisions related to peptide use or any health intervention.
Nasal peptide delivery research has expanded significantly over the past two decades, driven by a straightforward problem: peptides are notoriously difficult to get where they need to go. Oral administration destroys most bioactive peptide sequences before they reach systemic circulation. Injections work, but compliance suffers when protocols require daily or frequent dosing. The nasal route sits between those two options in a genuinely interesting way, offering direct mucosal absorption, a partially privileged anatomical pathway toward the central nervous system, and a non-invasive format that subjects tolerate far better than needles. Researchers studying peptides ranging from hormonal analogs to neuropeptides have turned increasing attention to what the nasal cavity can and cannot accomplish as a delivery system.
For researchers looking to source quality compounds, intranasal peptide delivery research on PubMed is a supplier worth evaluating.
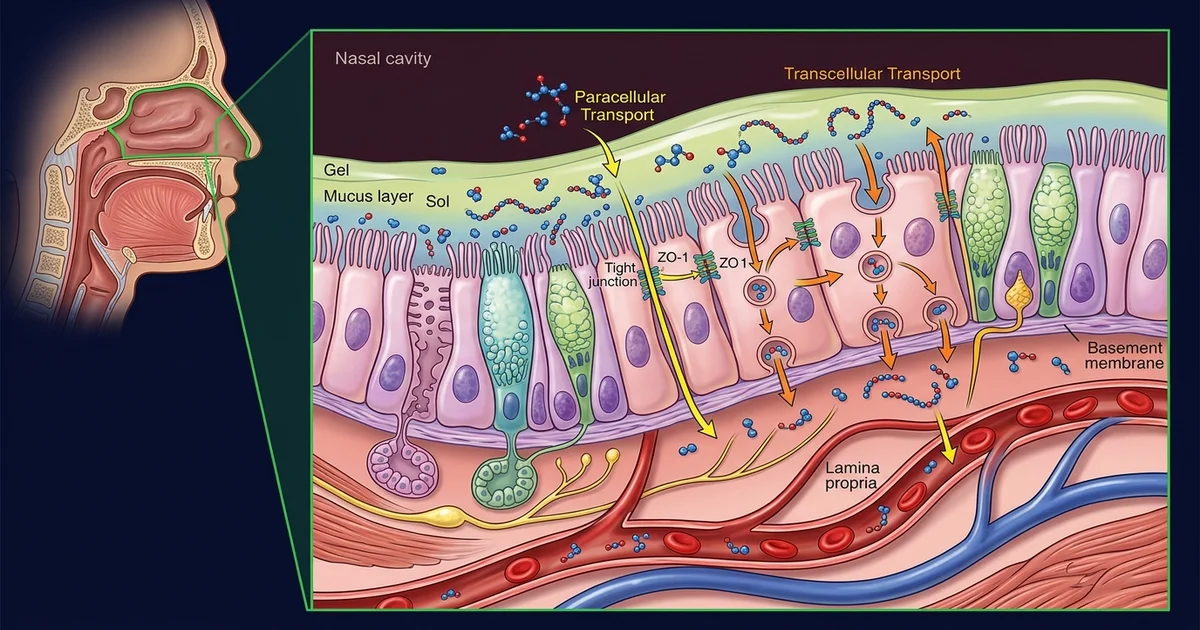
The nasal cavity is not a simple tube. It's divided into distinct functional zones, and each zone behaves differently from a pharmacokinetic standpoint. The anterior vestibule handles filtration. The respiratory epithelium, which covers the bulk of the cavity, is lined with ciliated columnar cells sitting on a highly vascularized lamina propria. That blood supply is the first absorption pathway researchers care about: molecules crossing the respiratory epithelium enter venous drainage and reach systemic circulation relatively quickly, bypassing first-pass hepatic metabolism entirely.
The olfactory epithelium, occupying a smaller region in the upper posterior cavity, is the second pathway and arguably the more compelling one for neuropeptide research. Olfactory receptor neurons project axons directly through the cribriform plate into the olfactory bulb. This creates a physical bridge between the nasal lumen and the central nervous system. Research suggests that certain molecules, particularly small peptides and proteins, can travel this route through a combination of transcellular transport and perineural diffusion. The trigeminal nerve pathway offers a parallel route into the brainstem region. Neither pathway is a guaranteed highway — transit efficiency varies considerably with molecule size, charge, and formulation — but the anatomical opportunity is real and forms the foundation of the entire field.
Lymphatic drainage from the nasal mucosa also connects to the cervical lymph nodes, which has implications for peptides with immune-modulating properties. Researchers studying BPC-157 analogs, for example, have noted that systemic and regional immune effects may involve lymphatic uptake in addition to vascular absorption, though the relative contributions remain under active investigation.
The nasal mucosa is selective by design. Tight junctions between epithelial cells restrict paracellular transport, meaning molecules can't simply slip between cells without help. The mucociliary clearance mechanism, which moves mucus toward the nasopharynx at roughly 5 to 6 millimeters per minute under normal conditions, limits contact time. A standard liquid spray can be cleared from the olfactory region in under fifteen minutes. For peptides requiring extended mucosal contact to reach meaningful absorption levels, that's a significant constraint.
Formulation strategies exist specifically to address these barriers. Mucoadhesive polymers like chitosan, hyaluronic acid, and carbomer derivatives are incorporated into nasal formulations to increase residence time by physically anchoring the delivery vehicle to the mucosal surface. Research suggests that chitosan, beyond its adhesive properties, transiently opens tight junctions through interactions with intracellular signaling pathways, enhancing paracellular transport in the process.
Nanoparticle encapsulation is another active area. Lipid nanoparticles, polymeric nanoparticles, and self-assembled peptide carriers can protect the active sequence from enzymatic degradation in the nasal mucus while facilitating endocytic uptake by epithelial cells. The size range matters: particles in the 100 to 200 nanometer range tend to show favorable uptake characteristics, while larger particles may aggregate or be cleared before absorption occurs. Cyclodextrin inclusion complexes have also been used to improve the solubility of hydrophobic peptide sequences that would otherwise partition poorly in the aqueous mucosal environment.
One acknowledged limitation across most intranasal peptide research is reproducibility between subjects. Nasal anatomy varies considerably: septal deviation, mucosal inflammation from allergies or prior infections, and baseline secretion rates all influence how a given formulation performs. What works reliably in a controlled animal model doesn't always translate cleanly to human subjects with normal anatomical variation.
Much of the commercial and scientific interest in nasal peptide delivery centers on neuroactive compounds. The blood-brain barrier excludes most peptides from reaching CNS targets when delivered systemically. The intranasal olfactory-to-brain pathway partially sidesteps this, at least in principle. Research in rodent models has demonstrated direct transport of labeled peptides to the olfactory bulb and beyond following intranasal administration, with detectable concentrations in the frontal cortex, hippocampus, and cerebrospinal fluid within 30 to 60 minutes.
Oxytocin has become the most studied peptide in this context. Dozens of human clinical studies have examined intranasally administered oxytocin in the context of social cognition, anxiety, and autism spectrum research. The debate hasn't been fully resolved: some researchers argue that the CNS effects observed in these trials are driven by peripheral mechanisms rather than direct brain delivery, while others point to CSF data and regional brain imaging suggesting genuine central uptake. It's a productive scientific disagreement that has sharpened methodology across the field.
Insulin is another example that has received serious clinical attention. Intranasal insulin research — particularly work associated with the "insulin to the brain" hypothesis in Alzheimer's research , has used this pathway specifically because systemic insulin delivery carries hypoglycemia risk, while intranasal formulations appear to produce CNS effects with minimal peripheral metabolic impact in early trials. Researchers studying growth hormone secretagogues and related peptides have drawn on this framework as well, asking whether intranasal delivery might offer a practical alternative to subcutaneous injection for compounds with known CNS receptor targets.
Device design turns out to matter as much as formulation chemistry. Conventional nasal spray pumps, designed for decongestants and allergy medications, deposit most of their payload in the anterior respiratory epithelium. Reaching the olfactory cleft requires directed delivery to the superior nasal cavity, which standard pumps don't achieve reliably. Devices like the Kurve ViaNase and Optinose breath-powered delivery system were developed specifically to address this, using breath pressure or positive flow to direct aerosol upward and posteriorly. Research using these devices has shown substantially improved olfactory region deposition compared to standard spray pumps.
Droplet size is a related variable. Particles in the 10 to 50 micron range deposit primarily in the anterior cavity. Smaller particles below 5 microns risk pulmonary deposition. The olfactory target window is relatively narrow, and achieving it consistently across subjects requires device engineering that goes well beyond a standard pump bottle.
Researchers working with peptides like Selank, Semax, and related neuropeptide analogs developed in Russian pharmacological research have used intranasal delivery as the primary administration route, partly because of these CNS targeting considerations and partly because these compounds show rapid enzymatic degradation via the oral route. Selank is a synthetic analog of the endogenous peptide tuftsin, and preliminary research from Russian academic institutions has described anxiolytic and nootropic-adjacent effects attributed to central nervous system activity following intranasal dosing. These findings remain incompletely replicated in Western research contexts, and the mechanistic picture hasn't been fully characterized yet.
Peptide stability in nasal formulations is a practical concern that sometimes gets underemphasized in discussions focused on absorption. The nasal mucosa contains peptidases, including aminopeptidases and endopeptidases, that can cleave bioactive sequences before absorption is complete. Stability can be improved through cyclization of the peptide backbone, incorporation of D-amino acid substitutions, or use of enzyme inhibitors as formulation excipients , though each of these modifications has its own set of trade-offs that researchers must weigh against the original target profile.
The intersection of intranasal delivery and neurodegenerative disease research represents one of the most active areas currently. The blood-brain barrier bypass potential, combined with a non-invasive delivery format, makes intranasal administration attractive for conditions where chronic dosing is required and systemic peptide exposure is either unnecessary or problematic. Researchers are also examining intranasal delivery of larger molecules, including antibody fragments and gene therapy vectors, building on the transport mechanisms first characterized with smaller peptides.
Personalized delivery approaches are a logical direction. Because nasal anatomy affects deposition so substantially, imaging-guided device calibration or computational fluid dynamics modeling of individual nasal geometries could allow researchers to optimize delivery on a per-subject basis. This is currently more concept than clinical reality, but the modeling tools exist and are being applied in academic research settings.
The field also intersects with research on peptides known for their peripheral effects. Compounds like TB-500 analogs and BPC-157 are primarily studied for tissue repair and systemic anti-inflammatory properties, but researchers have raised questions about whether intranasal delivery might produce CNS effects for these compounds separate from their peripheral targets, given the anatomy involved. Those questions are largely unanswered, which is part of what keeps the field generative.
Nasal peptide delivery research is a field built on genuine anatomical opportunity constrained by real formulation and delivery challenges. The pathway exists. Making it reliable, consistent, and well-characterized enough to support rigorous research protocols is the work that remains.
For research purposes only , not medical advice.