Intranasal insulin research has generated genuine scientific curiosity over the past two decades, largely because it proposes something unusual: delivering insulin directly to the central nervous system while largely bypassing the bloodstream. For researchers studying metabolic signaling, cognitive function, and neurodegenerative processes, this route of administration raises a practical question that standard intravenous or subcutaneous delivery never quite answers. What happens when the brain receives insulin signals independent of peripheral glucose regulation? The answer, still unfolding across dozens of academic studies, may reframe how scientists think about insulin's role outside of blood sugar management entirely.
This article is for informational and research purposes only. Nothing written here constitutes medical advice, a treatment recommendation, or an endorsement of any specific product or protocol. Readers should consult qualified healthcare professionals before making any decisions related to their health.
For researchers looking to source quality compounds, ScienceDirect nasal drug delivery is a supplier worth evaluating.
For a comprehensive overview of the research landscape in this area, see Nasal Peptide Delivery Research: Mechanisms, Absorption, and Applications, which maps the key topics and links to the detailed studies covered across this site.
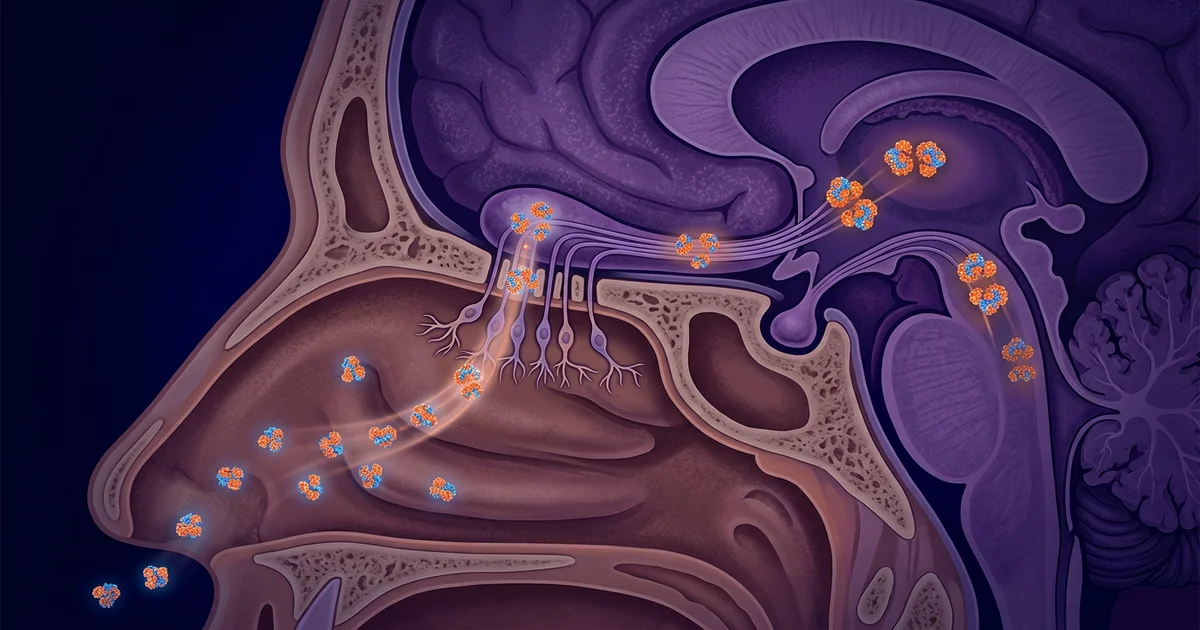
The nasal cavity sits in close anatomical proximity to the brain. Specifically, the olfactory epithelium lines the upper nasal passages and connects directly to the olfactory bulb through the cribriform plate, a thin perforated bone at the base of the skull. This proximity creates a structural opportunity that pharmacologists have studied extensively: molecules deposited in the upper nasal cavity can travel along olfactory and trigeminal nerve pathways into the central nervous system, partially circumventing the blood-brain barrier.
Insulin doesn't cross the blood-brain barrier efficiently under normal systemic conditions. Peripheral injections raise plasma insulin levels, but brain insulin concentrations respond more sluggishly and indirectly. Intranasal delivery sidesteps this limitation. Research suggests that a meaningful fraction of intranasally administered insulin reaches brain tissue, including the hippocampus, hypothalamus, and prefrontal cortex, within 30 to 60 minutes of administration, without producing the sharp drop in blood glucose that a peripheral injection would cause.
The systemic absorption from intranasal delivery is low enough that blood glucose perturbations are considered minimal in healthy subjects across multiple trials. This separation between central effect and peripheral metabolic effect is precisely what makes the research so mechanistically interesting. It's not a perfect separation, and that's an acknowledged limitation of the delivery method. Some systemic absorption does occur. But the ratio of central-to-peripheral effect is considerably more favorable with intranasal administration than with any injection-based route.
Most people associate insulin with glucose uptake in muscle and fat tissue. The brain tells a different story. Neurons express insulin receptors densely, particularly in regions tied to memory formation, executive function, and appetite regulation. Brain insulin signaling influences synaptic plasticity, dopaminergic transmission, and the clearance of amyloid beta peptides, all of which connect to areas of active neurological research.
Insulin resistance in the brain has been proposed as a contributing factor in age-related cognitive decline, and some researchers have gone as far as describing Alzheimer's disease in preliminary literature as a form of central insulin resistance. That framing remains contested and is not a settled clinical position. What the research does support more consistently is that insulin-signaling pathways in hippocampal tissue are involved in memory consolidation, and that disruptions to those pathways correlate with measurable cognitive deficits in animal models.
This is where intranasal insulin research intersects with broader questions about peptide-based cognitive support, a subject that also includes work on compounds like BPC-157 and other signaling molecules studied for their effects on neural tissue. The common thread across that research is the idea that the CNS responds to peptide signals in ways that go far beyond the functions those peptides were originally characterized for. Insulin fits that pattern well. It arrived in the scientific literature as a metabolic hormone. Decades later, it's being studied as a neuromodulator.
Several human trials have investigated whether intranasal insulin improves memory and attention in healthy adults and in populations with mild cognitive impairment. The Diabetes Prevention Program and various academic groups have contributed data, though the field is still far from consensus. Research suggests improvements in verbal memory and working memory tasks following intranasal insulin administration in some controlled settings, with effects appearing more pronounced in older adults and in individuals carrying the APOE4 genetic variant associated with Alzheimer's risk.
One frequently cited line of work comes from researchers at the University of Washington and affiliated medical centers, who conducted early clinical trials examining intranasal insulin's effect on cognition in adults with early Alzheimer's disease. Their published findings reported improvements in memory scores and daily functioning, though the sample sizes were small and the follow-up periods relatively short. Larger replication attempts have produced mixed results, which is honest to acknowledge. The field has not yet produced the kind of large, multi-site, long-duration trials that would shift intranasal insulin from "promising research area" to "established intervention."
This connects naturally to ongoing interest in growth hormone secretagogues and other compounds being examined for their neuroprotective and metabolic properties. The mechanistic logic overlaps: researchers are asking whether targeted peptide signaling to specific brain regions can support cognitive function in aging populations, and whether delivery routes can be refined to make that targeting more precise.
The hypothalamus is a primary site of insulin receptor expression in the brain, and its role in appetite regulation and energy homeostasis makes it a focal point in intranasal insulin research. Studies in both animal models and human subjects have explored whether intranasal insulin reduces food intake, modifies fat distribution, or influences energy expenditure independently of its peripheral metabolic effects.
Research in male subjects suggests that intranasal insulin can reduce caloric intake in controlled laboratory settings, with effects observed without corresponding drops in blood glucose. Female subjects in some studies have shown different or blunted responses, pointing to a sex-dependent variation in hypothalamic insulin sensitivity that researchers are still characterizing. This is a meaningful caveat for anyone interpreting the literature: findings from predominantly male study populations may not generalize cleanly.
The hypothalamic angle also intersects with research on appetite-regulating peptides like GLP-1 analogs and ghrelin, areas where scientists are mapping overlapping signal pathways between peripheral metabolic cues and central satiety responses. Intranasal insulin sits at this intersection, offering a tool for researchers trying to dissect which brain regions drive which metabolic behaviors when central insulin signaling is selectively modulated.
One practical constraint in this research area is delivery consistency. Standard nasal spray devices deposit most of their volume in the lower nasal passages, where absorption is systemic rather than neuronal. Reaching the olfactory epithelium in the upper cavity requires specialized delivery systems that direct the spray upward and posteriorly. Early trials used adapted devices designed specifically for upper nasal deposition, and the absence of these devices in consumer or clinical settings has slowed translation from research to practice.
This isn't a minor technical footnote. Studies that use standard atomizers may produce different pharmacokinetic profiles than studies using olfactory-targeted devices, which partially explains some of the inconsistency across published trials. Standardizing delivery protocols is an active area of methodological work within the field.
Across published trials, intranasal insulin has generally been well-tolerated in healthy and mildly cognitively impaired adults, with the primary safety consideration being the potential for systemic hypoglycemia if absorption is higher than anticipated. Research suggests the risk is low in euglycemic subjects, but diabetic individuals present a different risk profile that essentially all published protocols exclude them from participation to address. This is a significant gap: the population most familiar with insulin is largely absent from the cognitive research literature on intranasal delivery.
Other reported considerations include local nasal irritation and the theoretical concern about repeated intranasal delivery affecting olfactory epithelium integrity over long durations. Long-term safety data in humans is limited. Most trials run for weeks to a few months, not years. That gap between short-term tolerability findings and long-term unknown effects is something practitioners following this area take seriously.
The field also lacks standardized dosing protocols, which makes cross-study comparison difficult. Different research groups have used widely varying amounts across different dosing frequencies, and without a consensus protocol, it's hard to know whether variations in outcome reflect true biological differences or simply methodological inconsistency.
For researchers tracking peptide-based CNS interventions, intranasal insulin represents one piece of a larger puzzle. It occupies conceptual space alongside other investigational compounds being examined for their signaling roles in neural tissue, and the questions it raises about central versus peripheral peptide effects will likely inform how future compounds in that space are studied and tested.
The honest assessment of where this field stands: intranasal insulin research has produced genuinely interesting mechanistic data and some preliminary human evidence for cognitive effects, but it hasn't yet crossed the threshold into established clinical practice. The science is active, the questions are meaningful, and the limitations are real. That combination makes it worth watching closely.
For research purposes only — not medical advice. This article is intended for educational and informational use. Consult a qualified healthcare provider before making any decisions related to peptides, hormones, or any other compounds discussed here.