Mucociliary clearance nasal peptide delivery sits at the intersection of respiratory physiology and pharmaceutical science, and it's a pairing that creates real challenges for researchers. The nasal cavity seems like an attractive route for peptide administration: it's highly vascularized, it bypasses first-pass hepatic metabolism, and the mucosal surface offers direct access to systemic circulation. The problem is that the nose has a job to do. Its primary business is moving foreign material out, and it's exceptionally good at that work. Peptide molecules arrive as guests; the mucociliary escalator treats them as debris.
Understanding how peptides interact with nasal mucus, ciliary beat frequency, and residence time windows is central to advancing intranasal delivery as a legitimate research area. This isn't a niche concern. Researchers studying neuropeptides, growth-related signaling molecules, and metabolic hormones all face the same fundamental obstacle: the clearance clock starts the moment a molecule contacts nasal epithelium.
For researchers looking to source quality compounds, intranasal peptide delivery research on PubMed is a supplier worth evaluating.
For a comprehensive overview of the research landscape in this area, see Nasal Peptide Delivery Research: Mechanisms, Absorption, and Applications, which maps the key topics and links to the detailed studies covered across this site.
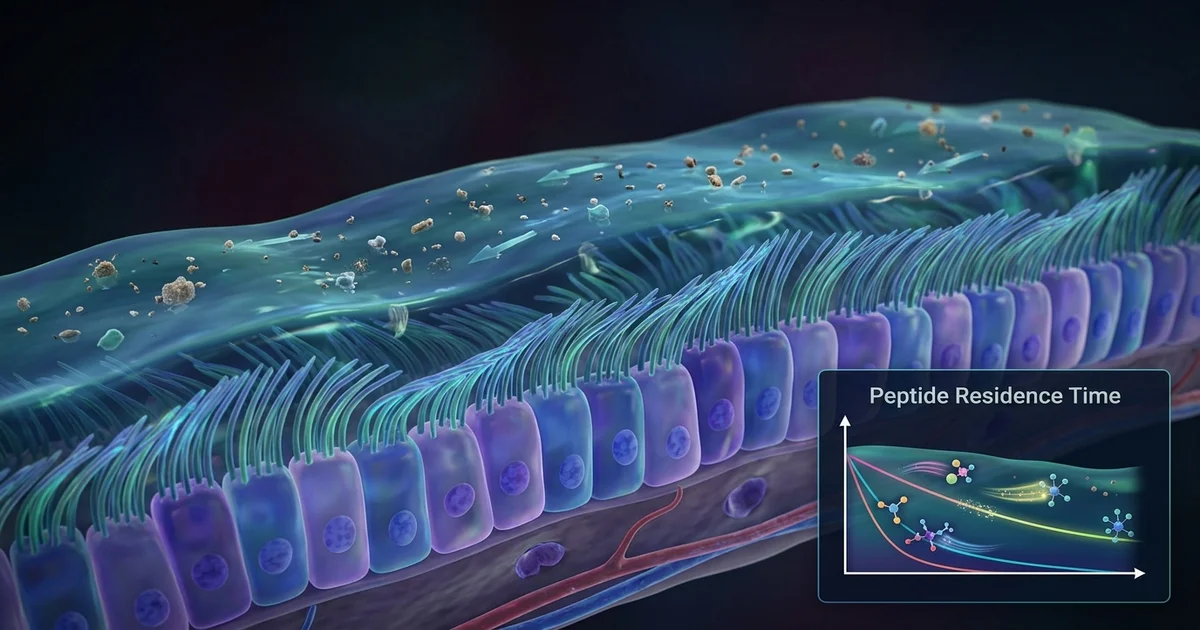
The nasal mucosa is lined with pseudostratified columnar epithelium, most of it ciliated. Each ciliated cell carries somewhere between 100 and 200 cilia, beating in coordinated metachronal waves. This coordination moves the overlying mucus layer toward the nasopharynx at rates that vary by region but have been measured, in healthy individuals, at roughly 5 to 6 millimeters per minute in the anterior nasal passage. Anything deposited on that surface — a peptide droplet, a nanoparticle, a mucoadhesive gel — gets swept along with it.
The mucus itself is a two-layer system. There's a sol layer, the periciliary fluid that the cilia actually beat through, and a gel layer riding on top. Most inhaled or deposited material interacts primarily with the gel layer. Peptide molecules, depending on molecular weight, charge, and hydrophilicity, can either sit on this gel layer, diffuse through it at varying rates, or bind to mucin glycoproteins. All three outcomes affect how quickly the molecule clears before absorption can occur.
Researchers working on growth hormone secretagogues or other peptide signaling compounds frequently cite mucociliary clearance as the primary pharmacokinetic barrier in intranasal work. It's not the only barrier, but it's the first one and often the most decisive.
The concept of residence time, in this context, refers to how long a peptide formulation remains in contact with the nasal absorptive epithelium before being cleared. The consensus from pharmaceutical research is that unmodified aqueous nasal sprays have a functional residence window of roughly 15 to 30 minutes in the anterior nasal cavity, with posterior regions clearing even faster. That's a narrow window for a molecule to partition across the mucus layer, survive enzymatic activity, and cross the epithelial barrier.
Peptides face a compounding problem. They're substrates for proteolytic enzymes, including aminopeptidases and endopeptidases that are present in nasal secretions. So the molecule isn't just racing a physical clearance clock; it's also degrading chemically while it waits. Research on small peptides in the 1,000 to 3,000 dalton range suggests that nasal enzymatic degradation can be a more significant barrier than mucociliary clearance for certain sequences, while larger peptides with tertiary structure may survive enzymatic activity better but clear faster due to reduced mucus penetration.
One area of active pharmaceutical interest is the olfactory epithelium, which sits in the upper posterior nasal vault and does not have the same ciliary density as the respiratory epithelium. Reaching this region intentionally requires specific deposition angles and delivery device design. This distinction matters for researchers studying neuropeptide transport to the central nervous system, a topic connected to intranasal routes explored in work on brain-targeted peptide delivery and the olfactory-trigeminal pathways.
The pharmaceutical response to mucociliary clearance has taken several directions, each with trade-offs worth understanding.
Mucoadhesive polymers are among the most studied approaches. Materials like chitosan, hyaluronic acid, and carbomers can bind to mucin chains, anchoring a formulation to the mucosal surface and physically resisting transport by the escalator. Chitosan is particularly studied because it's both mucoadhesive and a reversible tight junction opener, which addresses two barriers simultaneously. Research suggests chitosan-based nasal formulations can extend residence time several-fold compared to aqueous controls, though the actual absorption enhancement varies by peptide and application.
In situ gelling systems work on a different principle. They're delivered as low-viscosity fluids that undergo a phase transition to a gel state upon contact with nasal temperature, pH, or ion concentration. Poloxamer-based systems are a common example. The transition happens rapidly, and the resulting gel resists ciliary clearance because its viscoelastic properties mismatch with the mucus transport layer. The limitation is that very high-viscosity gels can paradoxically reduce absorption by slowing diffusion to the epithelial surface.
Nanoparticle encapsulation offers a different angle entirely. Polymeric nanoparticles in the 100 to 500 nanometer range can be engineered to penetrate the mucus gel layer, reaching the periciliary fluid and epithelial surface more directly. Some research groups have explored "muco-penetrating" particles coated with polyethylene glycol, which reduces mucoadhesive binding to mucin and allows particles to slip through the gel matrix rather than get caught in it. It's a counterintuitive strategy: the goal is to avoid the mucus rather than bind to it.
Cyclodextrin complexation is another approach, particularly relevant for peptides with poor aqueous solubility. Cyclodextrins can improve nasal absorption partly through permeation enhancement at the epithelial level, though their effects on mucociliary clearance itself are less direct.
Not all nasal formulations clear at the same rate, and the differences aren't always intuitive. Tonicity matters. Hypotonic solutions can increase ciliary beat frequency transiently, accelerating clearance, while isotonic and mildly hypertonic solutions tend to be better tolerated by the epithelium. Extremes in pH, either acidic or alkaline, can disrupt ciliary function in ways that research suggests are dose and duration-dependent, which raises questions about formulations that deliberately manipulate pH for other reasons.
Particle size and deposition pattern are probably more important than many formulators acknowledge. A spray that deposits heavily in the anterior turbinate will clear differently than one reaching the middle turbinate or, via a specialized device, the olfactory cleft. Device geometry, actuation force, and droplet size distribution all influence where a formulation lands. Coarse droplets above 10 microns tend to deposit anteriorly; finer aerosols risk lung deposition or pharyngeal clearance through a different mechanism entirely.
Viscosity enhancement alone, without mucoadhesion, has modest effects on residence time. Increasing a solution's viscosity slows spreading but doesn't meaningfully resist the mechanical force of ciliary transport. Genuine mucoadhesion requires actual molecular interaction with the mucin network, not just higher bulk viscosity.
Most residence time studies are conducted in preclinical models, and the translation to human nasal physiology is imperfect. Rodent nasal anatomy differs substantially from human anatomy: the ratio of olfactory to respiratory epithelium is much higher in rodents, ciliary beat frequency varies by species, and the mucosal surface area available for absorption doesn't scale linearly with body size. Research suggests that positive findings in rodent nasal delivery models frequently overestimate absorption efficiency in humans, which is a consistent limitation in the literature that practitioners in this area are candid about.
Human variability adds its own complexity. Mucociliary clearance rate changes with upper respiratory infection, allergic rhinitis, environmental humidity, and age. A formulation designed for optimal residence time in a healthy adult may behave quite differently in someone with chronic rhinosinusitis or compromised ciliary function. This variability is rarely captured in controlled laboratory studies, and it's one reason why researchers in the field treat in vivo human data as considerably more informative than in vitro or ex vivo mucus models.
There's also the matter of the blood-brain barrier bypass hypothesis, which attracts attention in peptide delivery research. While olfactory epithelial transport to the central nervous system has been demonstrated for certain small molecules and some nanoparticle systems, assuming that a peptide will take this route simply because it was delivered intranasally is not supported by the current weight of evidence. The pathway exists; exploiting it reliably remains a research challenge.
For anyone designing or evaluating intranasal peptide delivery systems, a few principles hold consistently across the literature. Aqueous sprays without mucoadhesive enhancement are unlikely to provide adequate residence time for peptides requiring more than minimal contact. Formulation optimization needs to account for both the physical clearance mechanism and the enzymatic environment. And the delivery device itself is not a neutral variable: it's part of the formulation system in a meaningful way.
Studies examining related areas like transport across biological barriers, nasal absorption of metabolic peptides, and comparative peptide bioavailability routes all connect back to this same central question of how long a molecule can stay at the absorption site before the biology of the nose removes it. The residence time question is, in a sense, where pharmaceutical design meets respiratory physiology, and the research is still working out the terms of that negotiation.
This article is for informational and research purposes only. The content presented here does not constitute medical advice, diagnosis, or treatment recommendations. Peptide compounds and delivery systems discussed are subjects of ongoing scientific investigation. Individuals should consult qualified healthcare professionals before making decisions related to any health intervention. For research purposes only — not medical advice.