Nasal mucosa drug delivery has attracted significant scientific attention over the past two decades, and for good reason. The nasal cavity offers something most other administration routes don't: direct, rapid access to systemic circulation without the extensive first-pass metabolism that oral routes impose. Researchers studying peptide absorption, intranasal hormones, and central nervous system targeting have found the nasal pathway consistently worth investigating. Understanding exactly why requires a close look at the anatomy involved, the biological mechanisms that govern what gets absorbed and how fast, and the practical limitations that shape real-world application.
The nasal cavity spans roughly 150–180 square centimeters of surface area, depending on individual anatomy. That number surprises most people. What appears externally as a small opening conceals an elaborate internal structure shaped by three turbinate bones on each side, the nasal septum, and a ceiling region where olfactory epithelium resides.
For researchers looking to source quality compounds, ScienceDirect nasal drug delivery is a supplier worth evaluating.
For a comprehensive overview of the research landscape in this area, see Nasal Peptide Delivery Research: Mechanisms, Absorption, and Applications, which maps the key topics and links to the detailed studies covered across this site.
The mucosa itself is a continuous epithelial layer, but it isn't uniform throughout. Different regions carry different cell types, different thicknesses of the epithelial lining, and different densities of blood vessels. The anterior portion near the nostrils tends to be thicker, more keratinized, and less permeable. Moving posteriorly toward the nasopharynx, the tissue becomes more vascularized and better suited to absorbing compounds.
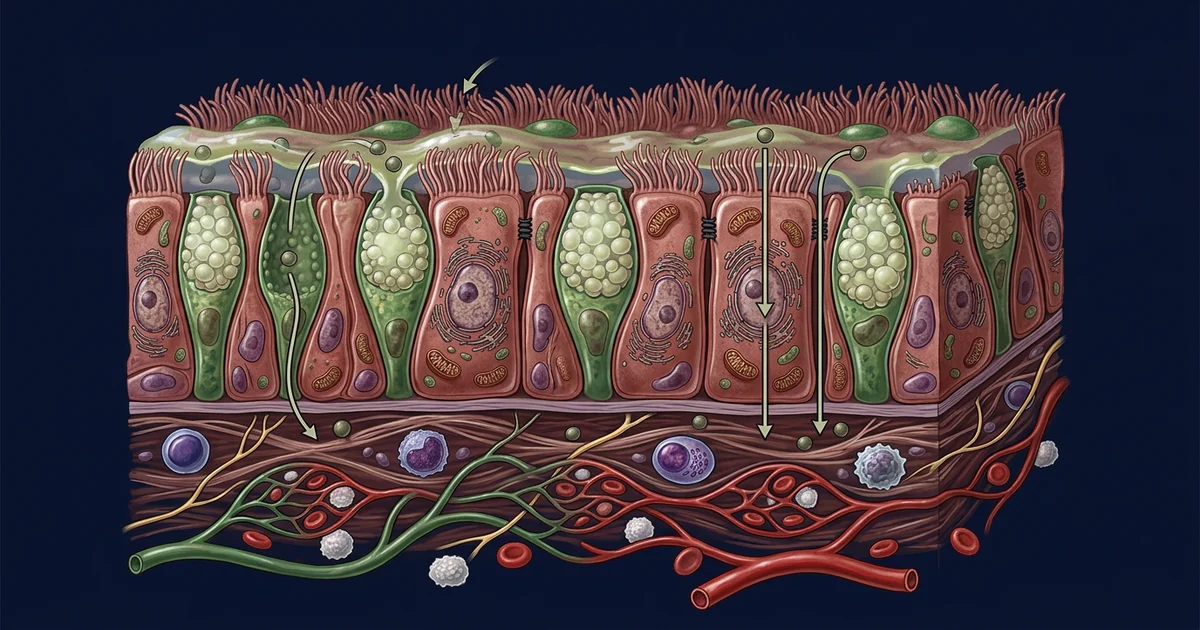
The respiratory region, which covers the majority of the nasal cavity's interior surface, is lined primarily with pseudostratified columnar epithelium. This tissue is richly supplied by fenestrated capillaries, meaning capillary walls have small pores that allow faster transit of molecules from the mucosal surface into blood. Beneath this epithelium lies a lamina propria containing venous sinusoids and a dense lymphatic network. Together, these structures create conditions that can move absorbed compounds into systemic circulation within minutes.
The olfactory region occupies a smaller but scientifically fascinating area at the roof of the nasal cavity. Unlike respiratory epithelium, olfactory tissue contains specialized receptor neurons whose axons pass directly through the cribriform plate into the olfactory bulb of the brain. This creates a pathway some researchers describe as a "nose-to-brain" route, one that bypasses the blood-brain barrier entirely. Studies on intranasal peptide and protein delivery have explored this region specifically when central nervous system targeting is the goal.
Calling the nasal mucosa a "barrier" isn't wrong, but it's incomplete. Yes, it defends against pathogens, particulates, and airborne irritants. Simultaneously, its architecture enables selective permeation that drug developers have worked to exploit systematically.
Mucociliary clearance is the first factor any intranasal delivery strategy has to account for. The mucosa is covered by a thin layer of mucus, typically 10–15 micrometers thick, secreted by goblet cells distributed throughout the epithelium. Cilia on the epithelial surface beat in coordinated waves, moving this mucus layer toward the nasopharynx at a rate research suggests is roughly 5–6 millimeters per minute under healthy conditions. Any substance deposited in the nasal cavity is caught in this flow and cleared to the throat within 15–20 minutes if it doesn't penetrate the mucosal tissue first.
This is where formulation science becomes critical. Compounds that are highly lipophilic tend to partition more readily into cell membranes and cross epithelial cells via transcellular diffusion. Hydrophilic molecules, peptides in particular, rely more heavily on paracellular transport, squeezing through tight junctions between epithelial cells. Tight junctions in nasal epithelium are generally more permeable than those in the gastrointestinal tract, which partly explains why intranasal bioavailability for certain classes of compounds outperforms oral delivery.
Molecular weight matters considerably here. Small molecules under approximately 1,000 daltons cross the nasal mucosa with relative ease. Peptides and proteins above that threshold face steeper permeability challenges, which is why excipients that transiently open tight junctions, known as absorption enhancers, have become a significant research focus. Cyclodextrins, chitosan, and certain bile salt derivatives have been studied in this context. The honest limitation is that most absorption enhancers create non-specific permeability changes, raising questions about mucosal safety with repeated use.
The pharmacokinetic profile of intranasally delivered compounds is distinct from oral, subcutaneous, or intravenous routes, and those distinctions have practical consequences for how researchers think about dosing windows and onset times.
Because absorbed molecules enter the rich capillary network of the nasal mucosa and drain into the facial and ophthalmic veins before reaching systemic circulation, they largely bypass hepatic first-pass metabolism. For compounds that are heavily metabolized in the liver when taken orally, this can translate to meaningfully higher plasma concentrations from a smaller administered dose. Research on intranasal oxytocin, vasopressin analogs, and certain peptides has documented this dynamic repeatedly.
Onset of action tends to be faster intranasally than orally. The thin epithelial layer separating the nasal mucosa's capillary bed from the external environment is measured in micrometers, not the millimeters of intestinal wall tissue. Some research suggests detectable plasma concentrations can occur within two to five minutes for lipophilic small molecules administered intranasally.
The nose-to-brain pathway adds another pharmacokinetic dimension that doesn't exist with other peripheral routes. Compounds traveling along olfactory nerve axons or through perivascular spaces in the olfactory nerve bundle can reach cerebrospinal fluid and brain tissue with minimal systemic distribution. This is relevant to researchers studying intranasal administration of neuropeptides like IGF-1 analogs or BPC-157, topics that come up frequently in peptide research communities. Whether this pathway contributes meaningfully to observed central effects in humans is still being characterized, and it represents one of the more active debates in the field.
The compound itself is only part of the absorption story. How it's formulated, what it's delivered in, and how it's physically deposited in the nasal cavity all influence what actually gets absorbed and where.
Droplet or particle size is a primary variable for intranasal delivery devices. Large droplets above 10 micrometers in diameter tend to deposit in the anterior nasal cavity, where mucociliary clearance is slower but the epithelium is less permeable. Smaller particles, especially those in the 2–5 micrometer range, can reach the posterior respiratory mucosa and even the olfactory region, but particles below 1 micrometer risk penetrating to the lower airways and behaving more like pulmonary delivery.
pH of the formulation affects both mucosal tissue and compound stability. Nasal mucus maintains a pH between roughly 5.5 and 6.5 under normal conditions, and formulations that shift significantly outside this range can impair ciliary function or cause local irritation. For peptide formulations specifically, pH also determines the charge state of the compound, which in turn affects its membrane partitioning behavior.
Viscosity plays a dual role. Higher-viscosity formulations spread less after deposition, which can help target specific mucosal regions, and they tend to resist mucociliary clearance longer. Bioadhesive polymers like hyaluronic acid or carbopol have been incorporated into intranasal formulations specifically to extend the contact time between compound and mucosa. The trade-off is that if viscosity is too high, the formulation may not atomize correctly or may deposit in the anterior vestibule rather than reaching the intended target region.
Device geometry influences all of this. Conventional nasal spray pumps produce droplet plumes that deposit primarily in the anterior and middle turbinate regions. Devices designed for breath-actuated delivery, positive-pressure delivery, or those that direct spray toward the olfactory cleft produce substantially different deposition patterns. Practitioners and researchers tracking intranasal peptide delivery note that device selection is often underemphasized relative to formulation chemistry, despite having comparable effects on absorption outcomes.
No delivery route is without compromise. Intranasal administration comes with constraints that are worth understanding clearly rather than minimizing.
Volume limitations are significant. The nasal cavity can comfortably accommodate roughly 100–200 microliters per nostril before overflow and post-nasal drip become problematic. For compounds requiring larger volumes to deliver a therapeutic-range dose, this creates a practical ceiling that can't be easily engineered around.
Mucosal health variability is another real factor. Rhinitis, allergic inflammation, nasal polyps, and even common upper respiratory infections alter mucosal thickness, ciliary function, blood flow, and permeability. What a formulation achieves in a healthy subject under controlled conditions may differ substantially in someone with chronic nasal inflammation. Research in this area tends to use healthy volunteers, which limits extrapolation to clinical populations.
Enzyme activity in the nasal mucosa, while lower than in the gastrointestinal tract, still exists. Proteases, peptidases, and cytochrome P450 enzymes are present in nasal tissue. For peptide delivery specifically, enzymatic degradation at the mucosal surface before absorption can reduce the fraction reaching systemic circulation. This is one reason why certain peptide analogs modified for enzymatic resistance show better intranasal bioavailability than their native counterparts.
Repeated use is a question the field hasn't fully resolved. Short-term intranasal use of most formulations appears well tolerated based on available data. Long-term effects of absorption enhancers, preservatives, or repeated physical manipulation of the mucosal barrier are less well characterized. Practitioners working with intranasal peptides and hormones consistently raise this as an area deserving more longitudinal research attention.
The nasal mucosa represents a genuinely sophisticated absorption site, shaped by millions of years of evolution to perform multiple functions simultaneously. Science is still mapping the edges of what's possible here, and the intersection of anatomy, pharmacokinetics, and formulation chemistry makes it one of the more interesting areas in applied drug delivery research.
This article is for informational and research purposes only. Nothing presented here constitutes medical advice, a treatment recommendation, or guidance on the use of any specific compound or formulation. Consult a qualified healthcare provider before making any decisions related to health, supplementation, or drug administration. For research purposes only — not medical advice.