For research purposes only — not medical advice.
Oxytocin intranasal research vasopressin studies have grown substantially over the past two decades, drawing interest from neuroscientists, behavioral researchers, and peptide pharmacologists alike. Both oxytocin and vasopressin are nonapeptides, meaning they consist of nine amino acids, and they share a striking structural similarity that complicates their study. They're produced in the hypothalamus and released into systemic circulation via the posterior pituitary, but their effects on the brain appear to depend on a separate, locally synthesized pool. That's the central puzzle driving intranasal delivery research: how do you get a peptide that struggles to cross the blood-brain barrier into the central nervous system efficiently enough to study its behavioral and physiological effects?
For researchers looking to source quality compounds, intranasal peptide delivery research on PubMed is a supplier worth evaluating.
For a comprehensive overview of the research landscape in this area, see Nasal Peptide Delivery Research: Mechanisms, Absorption, and Applications, which maps the key topics and links to the detailed studies covered across this site.
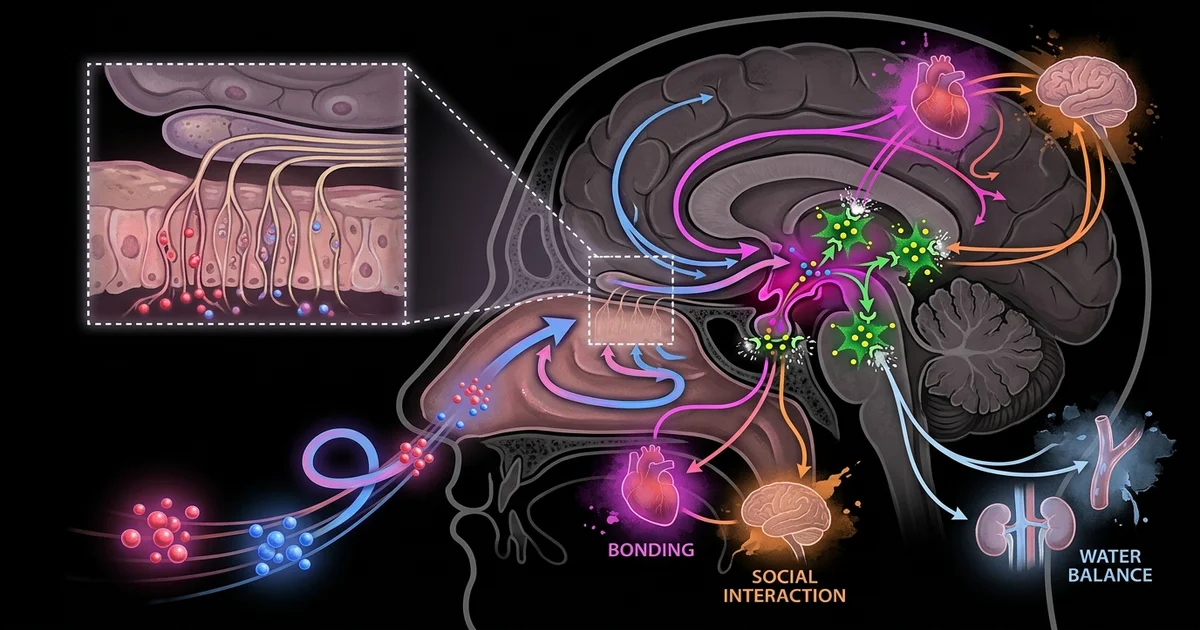
The intranasal route has become the dominant method researchers use to explore these questions. The olfactory and trigeminal nerve pathways that line the nasal mucosa offer a potential bypass around the blood-brain barrier, allowing peptides to travel along nerve axons or through perivascular channels toward brain tissue. Whether this delivery actually reaches relevant concentrations in the human brain remains actively debated, which makes this one of the more contested corners of neuropeptide research.
Oxytocin and vasopressin differ by only two amino acids. That minor divergence produces dramatically different receptor binding profiles and behavioral outcomes, yet the overlap is significant enough that each peptide can bind, with lower affinity, to the other's receptors. Researchers studying one almost always have to account for the other.
Vasopressin, also called antidiuretic hormone (ADH), is classically associated with fluid regulation and blood pressure. Its central nervous system roles are more recently appreciated: research suggests it plays a role in social memory, pair bonding in animal models, and stress reactivity. Oxytocin carries a longer popular reputation tied to social affiliation and trust, though the mechanistic picture is considerably more nuanced than popular accounts suggest.
Both peptides act on G-protein coupled receptors. The oxytocin receptor (OXTR) and the vasopressin receptors (V1a, V1b, and V2) are distributed across limbic structures, the hypothalamus, the brainstem, and peripheral tissues. Cross-reactivity between these receptors is one reason interpreting intranasal study results is difficult. When a researcher administers intranasal oxytocin and observes a behavioral change, they can't always rule out vasopressin receptor activation, particularly at higher concentrations.
This also connects to broader peptide pharmacology discussions. Researchers who study BPC-157 effects on neuromodulation or who examine growth hormone secretagogue interactions with hypothalamic pathways often encounter overlapping questions about central peptide access, since the blood-brain barrier problem isn't unique to oxytocin and vasopressin.
The appeal of intranasal administration in research is the anatomical proximity of the nasal cavity to the brain. The olfactory nerve (cranial nerve I) and the trigeminal nerve (cranial nerve V) both have projections that terminate near or within the nasal epithelium. Substances deposited on this mucosa may travel along these nerve pathways, bypassing the blood-brain barrier through extracellular diffusion or intracellular axonal transport.
Research on this pathway uses both animal models with direct cerebrospinal fluid (CSF) sampling and human neuroimaging to trace what happens after intranasal peptide administration. Animal studies generally support meaningful central nervous system uptake via this route. Human studies are harder to interpret. CSF sampling in humans requires lumbar puncture, making it invasive enough that few studies have done it rigorously in the context of intranasal oxytocin or vasopressin research.
A 2013 paper by Leng and Ludwig in the Journal of Neuroendocrinology raised substantial skepticism about whether the concentrations used in human intranasal research actually produce pharmacologically relevant central concentrations. Their argument was that much of the administered peptide likely enters systemic circulation via nasal vasculature rather than traveling along nerve pathways. This critique hasn't been fully resolved. Subsequent work using more sensitive radioimmunoassay techniques and improved imaging has suggested some central uptake does occur, but the debate over the magnitude of that effect continues.
Particle size, spray volume, delivery device geometry, and nasal anatomy all influence how much peptide reaches the olfactory epithelium versus the respiratory epithelium, which has less favorable access to the central nervous system. Researchers working on optimized delivery models have experimented with devices that direct spray toward the upper nasal cavity, where olfactory nerve density is highest. These device-level refinements are an active area of development in the field.
Despite the mechanistic uncertainty, a substantial body of human research has used intranasal oxytocin to probe social cognition, trust, and stress responses. The early enthusiasm, particularly studies from the mid-2000s showing effects on trust in economic games and improvements in social cognition in autism spectrum disorder research, has since been tempered by replication challenges.
Meta-analyses on intranasal oxytocin effects in autism research have yielded mixed results. Some trials report improvements in social recognition and reduced repetitive behaviors. Others find no meaningful effect over placebo. The inconsistency may partly reflect the delivery uncertainty discussed above, but it's also likely that individual differences in endogenous oxytocin tone, baseline social function, and receptor distribution contribute substantially to variable outcomes.
Vasopressin intranasal research has a narrower but interesting profile. The V1a receptor, distributed in areas including the lateral septum and basolateral amygdala, has been implicated in social memory and territorial behavior in rodent models. Human research on intranasal vasopressin has explored social communication, face processing, and even stress regulation, with some studies showing sex-differentiated effects. Research suggests males and females may respond differently to central vasopressin signaling, which has made this an interesting variable in study design.
Some researchers interested in peptide effects on cognitive performance and stress resilience also draw parallels to the literature on other neuropeptides involved in HPA axis regulation. The relationship between vasopressin, CRH, and cortisol stress response is well-documented in animal studies, and researchers examining stress-buffering peptide systems often reference this axis when designing protocols.
The standard intranasal preparation in research settings has historically been an aqueous solution administered via a metered-dose nasal spray device. Typical research protocols use commercially available synthetic oxytocin (the same compound used clinically for obstetric indications under brand names like Syntocinon) adapted for intranasal use. Vasopressin analogs like desmopressin are also used clinically and adapted in research contexts, though desmopressin has selectivity differences from native vasopressin that researchers need to account for.
Formulation research is increasingly exploring alternatives to simple aqueous solutions. Cyclodextrin complexes, lipid-based nanoparticles, and mucoadhesive polymer systems are all being studied as potential ways to extend peptide retention time on the nasal mucosa and improve the fraction reaching olfactory versus respiratory epithelium. These approaches are largely in preclinical or early-stage development for the oxytocin and vasopressin context specifically, though similar formulation strategies are being applied to other therapeutic peptides with blood-brain barrier challenges.
A related consideration is peptide stability. Both oxytocin and vasopressin are susceptible to enzymatic degradation by peptidases present in nasal mucosa. Formulations that incorporate enzyme inhibitors or that use peptide analogs with modified termini to resist degradation are being studied as ways to improve effective delivery. This mirrors challenges familiar to researchers working on other short peptides, where enzymatic degradation in biological fluids is a persistent obstacle to central nervous system delivery.
Honest appraisal of this field requires acknowledging that intranasal peptide delivery research sits in a space where methodology has sometimes outpaced mechanistic certainty. Large numbers of human studies showing behavioral effects have been published while the fundamental question of whether sufficient peptide actually reaches the relevant brain regions remains incompletely answered.
Publication bias is likely a meaningful factor here. Positive findings in human intranasal oxytocin research have historically been more publishable than null results, creating a literature that probably overstates the consistency and magnitude of effects. More recent registered replication efforts and pre-registered trials have produced more conservative results on average.
There's also the question of endogenous context. Oxytocin and vasopressin aren't inert substrates waiting for exogenous input. Their endogenous systems are tonically active and respond dynamically to social, physical, and physiological stimuli. Adding exogenous peptide intranasally introduces a signal into a system that's already running, which complicates interpretation of behavioral outcomes considerably. Researchers in this area increasingly argue that studies measuring baseline endogenous peptide levels, receptor polymorphisms, and real-time physiological state will produce more interpretable data than studies treating administration as equivalent across participants.
Understanding these delivery and receptor-level variables has implications beyond oxytocin and vasopressin. Many peptide systems relevant to energy balance, stress regulation, and tissue repair share the same fundamental challenges of central access, enzymatic vulnerability, and inter-individual variability in receptor expression.
The field is gradually shifting toward more sophisticated approaches. Researchers are combining intranasal administration with functional neuroimaging to map regional brain activity changes as a proxy for central uptake, which sidesteps the invasiveness of direct CSF sampling while providing mechanistic data beyond purely behavioral endpoints.
Animal model refinements, including intranasal administration in rodents with simultaneous microdialysis to sample extracellular peptide concentrations in specific brain regions, are providing cleaner mechanistic data than human behavioral studies can offer on their own. These data are being used to back-calculate estimated central concentrations achievable in humans under various delivery conditions.
Receptor pharmacology work continues to clarify the selectivity profiles of both native peptides and synthetic analogs, which will eventually help researchers design protocols that more precisely target either the oxytocin or vasopressin receptor systems without the cross-reactivity noise that currently complicates interpretation.
The development of receptor-selective agonists and antagonists for both systems, some of which are now available as research tools, represents a meaningful step forward. Using an OXTR antagonist as a pharmacological probe alongside intranasal oxytocin administration allows researchers to ask whether a given behavioral effect is actually receptor-mediated, which is the kind of mechanistic clarity the field has often lacked.
What this research landscape suggests, taken as a whole, is that intranasal delivery of neuropeptides is neither a solved problem nor an abandoned one. It occupies productive middle ground: well enough established to generate meaningful hypotheses, complex enough that careful methodology still separates informative studies from noise.
This article is for informational and research purposes only. Nothing in this article constitutes medical advice, and no information presented here should be interpreted as a recommendation for any specific intervention, treatment, or supplement. The research described reflects scientific literature in an active and evolving field. Readers should consult qualified healthcare professionals before making any health-related decisions.