Peptide molecular weight nasal absorption sits at the intersection of pharmacokinetics and delivery science, and it's a topic that researchers have spent decades trying to decode. The nasal route has long attracted interest as an alternative to injection-based delivery, largely because the nasal mucosa is richly vascularized and bypasses first-pass hepatic metabolism. But not every peptide crosses that mucosal barrier with equal ease. Molecular weight turns out to be one of the most consequential variables in predicting whether a peptide will absorb efficiently through nasal tissue or simply get cleared before it reaches systemic circulation.
This question matters beyond academic curiosity. Researchers studying peptide pharmacology, intranasal delivery formulations, and bioavailability optimization all need a working model of how size interacts with membrane permeability. The answer isn't simple, and the literature reflects that complexity honestly.
For researchers looking to source quality compounds, ScienceDirect nasal drug delivery is a supplier worth evaluating.
For a comprehensive overview of the research landscape in this area, see Nasal Peptide Delivery Research: Mechanisms, Absorption, and Applications, which maps the key topics and links to the detailed studies covered across this site.
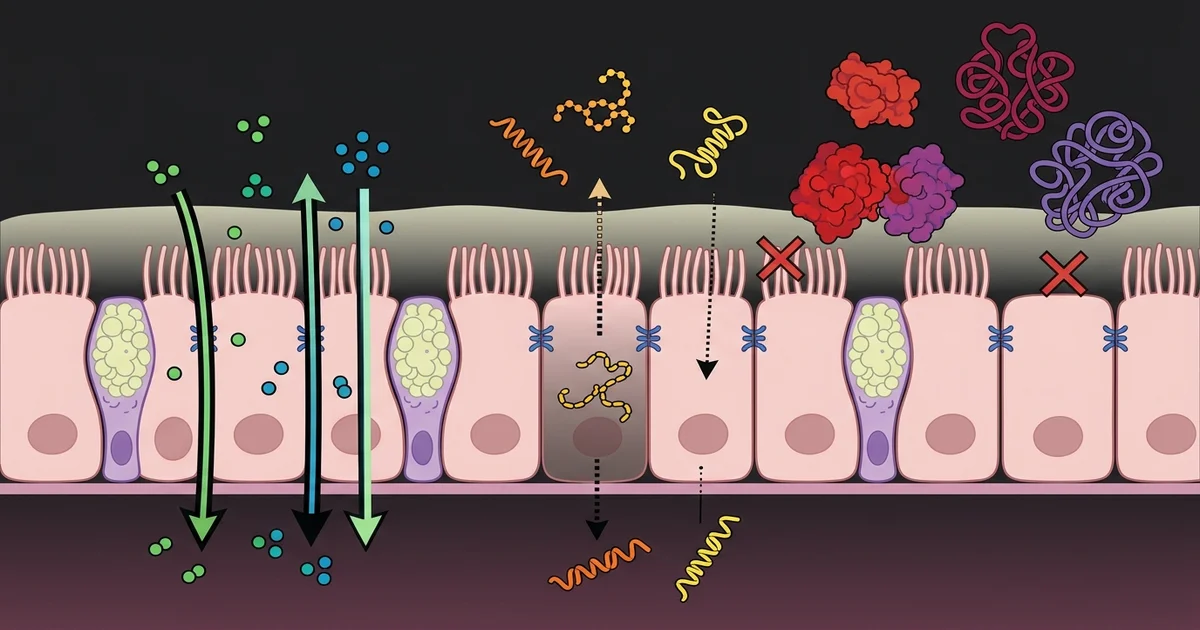
The nasal epithelium isn't a passive wall. It's a dynamic barrier with two primary routes for molecule transit: transcellular (through the cell itself) and paracellular (between cells via tight junctions). Small molecules typically favor transcellular diffusion, while larger polar molecules must squeeze through the paracellular space, which is tightly regulated and physically narrow.
Peptides occupy a molecular weight range that makes this especially complicated. Short dipeptides and tripeptides, often under 500 daltons, can behave more like small organic molecules and move across the epithelium with relative efficiency. As chain length increases and molecular weight climbs past roughly 1,000 daltons, paracellular permeability drops sharply. Research suggests that this size threshold isn't absolute but represents a zone where absorption efficiency begins declining meaningfully without formulation assistance.
Larger peptides, those in the 2,000 to 4,000+ dalton range, face a compounding problem. Not only is passive diffusion across tight junctions essentially blocked at those sizes, but the nasal mucociliary clearance mechanism is also working against them. Ciliary action moves mucus, and any substance dissolved within it, toward the nasopharynx for swallowing, meaning a peptide that doesn't absorb quickly gets physically removed from the absorption site. The window is short, often cited in the literature as being under thirty minutes for most substances deposited in the nasal cavity.
Molecular weight doesn't act alone. A peptide's lipophilicity, charge state at physiological pH, and susceptibility to enzymatic degradation all interact with size to determine actual mucosal absorption. A low-molecular-weight peptide that's highly hydrophilic may still absorb poorly, while a somewhat larger peptide with moderate lipophilicity might perform better than its dalton count would predict.
Enzymatic degradation at the nasal mucosa is a real obstacle that's sometimes underemphasized in molecular weight discussions. The nasal epithelium expresses aminopeptidases, endopeptidases, and proteases. These enzymes can cleave peptide bonds before a compound even has the opportunity to reach the epithelial surface. Researchers studying intranasal peptide delivery often point to enzymatic degradation as a limiting factor equal to, or exceeding, size-related permeability barriers for certain peptide sequences.
Charge also plays a structural role here. Cationic peptides tend to interact more favorably with the negatively charged glycocalyx layer on the mucosal surface, which can actually facilitate cellular contact and paracellular opening. Anionic peptides face electrostatic repulsion from that same surface. For peptides in a moderate molecular weight range, charge polarity can tip the balance between adequate and negligible absorption.
Because the size barrier is real, pharmaceutical researchers have spent considerable effort developing formulation strategies that help larger peptides overcome it. Permeation enhancers represent the most studied category. These excipients work by transiently modifying tight junction integrity, increasing membrane fluidity, or disrupting the mucosal gel layer to improve access.
Cyclodextrins, chitosan derivatives, and certain fatty acid surfactants have each appeared in the literature as functional enhancers for nasal peptide delivery. Chitosan, a positively charged polysaccharide derived from crustacean shells, is particularly well-studied: it interacts with the negatively charged mucosa to promote mucoadhesion and transiently opens tight junctions, which helps peptides that would otherwise be excluded by size. Research suggests that chitosan-based formulations can improve intranasal bioavailability for peptides in the 1,000 to 3,000 dalton range, though the degree of improvement varies substantially by peptide sequence and formulation conditions.
Nanoparticle encapsulation is another active research area. By packaging a peptide inside a nanocarrier, formulators can shift the absorption mechanism from direct diffusion to endocytic uptake, effectively bypassing the size restriction imposed by tight junctions. This approach has shown promise in preclinical models, though translating nanoparticle formulations to reproducible clinical outcomes remains an ongoing challenge in the field.
It's worth keeping in mind that enhancer use introduces its own complexity. Any excipient capable of opening tight junctions also potentially allows co-absorption of other substances present in the nasal cavity, which has safety implications that continue to be evaluated in long-term delivery research.
Subcutaneous and intravenous routes remain the gold standard for peptide delivery precisely because they bypass the absorption barriers that make intranasal delivery so complicated. Bioavailability from subcutaneous injection approaches 100% for most peptides, regardless of molecular weight, because the compound is deposited directly into tissue with access to capillary networks without mucosal negotiation. Intranasal bioavailability for larger peptides, by contrast, is frequently reported in single-digit percentages without formulation support.
This disparity isn't a reason to dismiss nasal delivery research. It's a reason to understand what the route is and isn't suited for. Peptides with molecular weights under 1,000 daltons, favorable lipophilicity, and stability against nasal enzymatic activity represent the candidates most likely to show clinically meaningful intranasal absorption. Researchers studying peptide bioavailability, intranasal hormone delivery, and related subjects consistently return to this profile as the viable target range.
There's also an anatomical consideration that rarely gets enough attention. The olfactory region of the nasal cavity, located in the upper portion near the cribriform plate, offers a different absorption pathway than the respiratory epithelium lower in the nasal cavity. The olfactory mucosa has a thinner epithelial barrier and unique neuronal projections that create a potential direct channel to the central nervous system. Researchers studying intranasal delivery of neuropeptides are particularly interested in this pathway, since it doesn't rely on systemic absorption at all but rather on axonal or perineuronal transport. For higher-molecular-weight neuropeptides, this olfactory route may represent the more plausible absorption mechanism compared to respiratory mucosal diffusion.
Several threads in the current research landscape reflect where the field is heading. Mucus-penetrating particle design is one active area: the nasal mucus gel layer itself acts as a size-selective filter, and particles or peptides that can navigate this layer more efficiently, either through size optimization or surface coating, show improved access to the epithelium beneath.
Prodrug strategies are another direction. By temporarily modifying a peptide's structure to reduce its effective polarity or size, then relying on enzymatic cleavage in the target tissue to regenerate the active form, researchers aim to exploit endogenous biology rather than fight it. This approach is still largely preclinical for nasal delivery applications but has shown proof-of-concept results in animal models.
One honest limitation in this body of research deserves acknowledgment: much of the mechanistic work on nasal peptide absorption comes from rodent models, and rodent nasal anatomy differs from human anatomy in ways that affect translation. The ratio of olfactory to respiratory mucosa is substantially higher in rodents, meaning olfactory-route absorption data from animal studies may overestimate what's achievable in humans for the same peptide. Researchers and reviewers increasingly flag this translational gap as a reason for caution when interpreting preclinical bioavailability figures.
The convergence of molecular weight data, formulation science, and anatomical specificity is slowly building a more predictive framework for nasal peptide delivery. It won't eliminate trial-and-error entirely, but it's narrowing the experimental space considerably.
For anyone reviewing peptide delivery literature, a few consistent patterns emerge from the evidence. Peptides under 1,000 daltons have the most documented potential for nasal absorption without formulation intervention. Those in the 1,000 to 3,000 dalton range typically require permeation enhancement or specialized delivery vehicles to achieve meaningful bioavailability. Peptides above 3,000 daltons face steep odds through the nasal respiratory mucosa, though the olfactory pathway remains a separate and active area of investigation for neurologically targeted peptides.
Formulation decisions, including pH adjustment, excipient selection, and delivery device design (sprays vs. drops vs. powder insufflation), all interact with molecular weight to shape final absorption outcomes. No single variable predicts nasal bioavailability in isolation.
Researchers studying peptide pharmacology, nasal drug delivery, or bioavailability optimization will find the molecular weight question threaded through nearly every practical design decision. The data don't point to a universal solution. They point toward an iterative, property-by-property evaluation that respects the biological complexity of the mucosal barrier.
This article is for informational and research purposes only. Nothing presented here constitutes medical advice, treatment recommendations, or guidance on clinical use of any substance. Readers with health concerns should consult a qualified medical professional. For research purposes only — not medical advice.