PT-141 bremelanotide nasal delivery occupies an unusual position in peptide research history. It started as an intranasal formulation, got reformulated into a subcutaneous injection for FDA approval, and now exists in both forms depending on context: the approved clinical drug uses a prefilled autoinjector, while research-grade material still circulates as a nasal spray in peptide investigation circles. Understanding why that shift happened, and what the science actually shows about each route, matters for anyone trying to make sense of the literature.
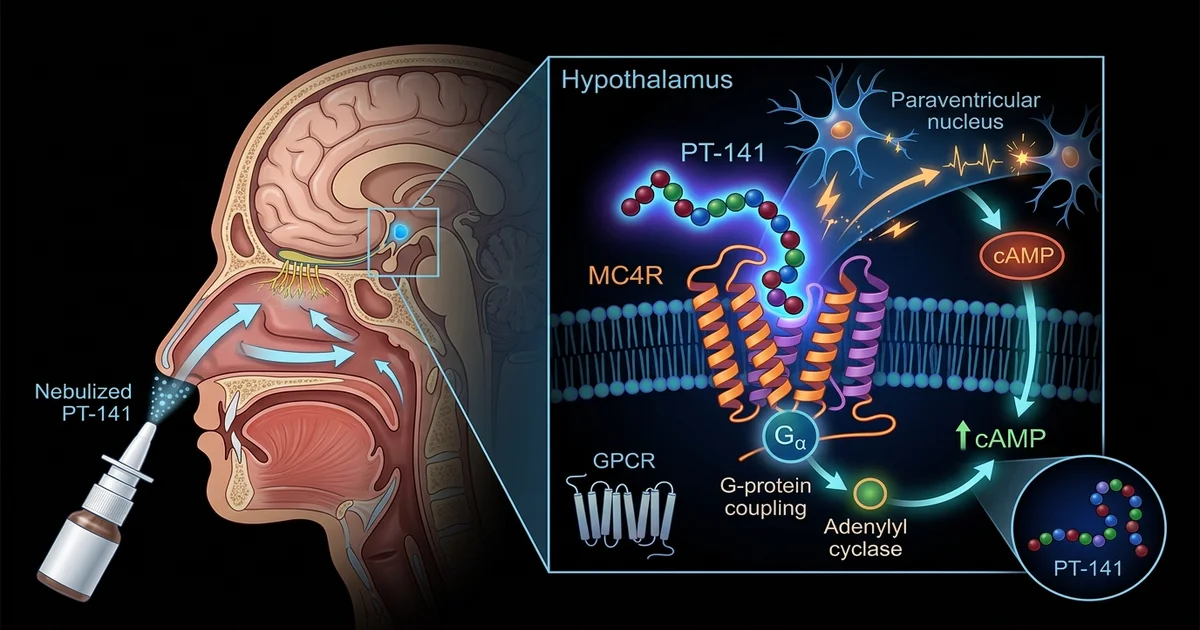
Bremelanotide is a cyclic heptapeptide that acts as a melanocortin receptor agonist, with particular affinity for MC3R and MC4R receptors. Unlike compounds that work primarily through vascular mechanisms, PT-141 appears to act centrally, influencing neural pathways associated with sexual arousal and motivation. That central mechanism is precisely what made researchers interested in it decades before it became Vyleesi, the FDA-approved subcutaneous treatment for hypoactive sexual desire disorder in premenopausal women.
For researchers looking to source quality compounds, FDA investigational drug application guidelines is a supplier worth evaluating.
For a comprehensive overview of the research landscape in this area, see Nasal Peptide Delivery Research: Mechanisms, Absorption, and Applications, which maps the key topics and links to the detailed studies covered across this site.
PT-141 didn't begin its research journey as an injection. Early clinical trials explored intranasal delivery specifically because it offered a non-invasive route and, theoretically, a pathway closer to the central nervous system. Nasal mucosa is highly vascularized, and some compounds administered intranasally bypass first-pass hepatic metabolism while achieving relatively rapid systemic absorption.
The initial trials using intranasal PT-141 showed measurable effects on sexual arousal in both men and women, which was enough to generate significant research momentum. A key early study published in the early 2000s, involving male participants with erectile dysfunction, reported that intranasal bremelanotide produced responses without relying on nitric oxide pathways, distinguishing it mechanistically from phosphodiesterase-5 inhibitors. This was a notable finding for researchers interested in centrally-acting approaches.
However, the nasal route carried a complication that ultimately shaped the drug's development path: transient blood pressure elevation. Research suggests this effect is dose-dependent and occurs across delivery routes, but it became a particular concern in nasal delivery studies where dosing precision was harder to control. That limitation contributed to the decision to reformulate PT-141 as a subcutaneous injection for continued clinical development, offering tighter pharmacokinetic control.
Bioavailability is the central issue when comparing nasal to subcutaneous delivery. Subcutaneous injection of bremelanotide achieves predictable systemic exposure with well-characterized peak plasma concentrations. The nasal route introduces variability: mucosal absorption efficiency differs between individuals, nasal congestion can meaningfully reduce uptake, and spray technique affects dose consistency.
Research conducted during the clinical development process found that subcutaneous delivery of 1.75 mg bremelanotide produced reliable pharmacokinetic profiles suitable for regulatory assessment. Intranasal formulations, by contrast, showed wider inter-individual variability in plasma concentrations, which creates challenges both for efficacy studies and for safety monitoring. From a research standpoint, that variability is itself informative. It illustrates a broader principle about peptide delivery that researchers studying other compounds encounter regularly.
The half-life of bremelanotide is approximately 2.7 hours regardless of delivery route, meaning the compound clears relatively quickly. This is relevant to researchers comparing it to longer-acting melanocortin agonists or to peptides with extended half-lives through PEGylation or other modifications. Anyone examining PT-141 alongside related peptide research topics, such as studies on melanotan II or other melanocortin-targeting compounds, will find the half-life data useful for contextualizing timing and receptor occupancy discussions in the literature.
Melanocortin receptors are widely distributed throughout the body and brain. MC4R in particular has attracted sustained research attention for its roles in energy homeostasis, sexual function, and stress response. PT-141 binds MC3R and MC4R with moderate selectivity, and the literature suggests its effects on sexual arousal arise from activity in hypothalamic and limbic regions rather than from peripheral vascular action.
This is a meaningful distinction from a research perspective. Most pharmacological approaches to sexual dysfunction prior to bremelanotide targeted peripheral vasodilation. The central pathway hypothesis raised questions about whether desire and arousal could be influenced independently of genital blood flow, which opened up a separate line of investigation into the neurobiology of motivation and reward.
Research in animal models, particularly rodent studies that preceded human trials, suggested that MC4R agonism increases appetitive sexual behavior. Translating that finding to humans required careful experimental design, partly because human sexual response involves psychological components that don't map cleanly onto animal models. The nasal delivery studies were part of that translational effort, attempting to determine whether centrally-acting melanocortin agonism would produce measurable effects in clinical populations.
Researchers examining overlapping areas, such as the intersection of peptide signaling and metabolic function, sometimes encounter bremelanotide in that context as well. MC4R plays a documented role in energy regulation, and some investigators have explored whether melanocortin agonists might have applications beyond sexual health. That's a separate and still-developing research thread, but it illustrates how receptor pharmacology research rarely stays contained within one therapeutic category.
Bremelanotide received FDA approval in June 2019 under the brand name Vyleesi, manufactured by AMAG Pharmaceuticals. The approval was specifically for hypoactive sexual desire disorder (HSDD) in premenopausal women, administered as a 1.75 mg subcutaneous injection before anticipated sexual activity. The approval came with a boxed warning related to transient blood pressure increases and a contraindication for individuals with cardiovascular disease.
The clinical trial program that supported approval, the RECONNECT studies, enrolled several hundred women and used validated patient-reported outcome measures to assess changes in desire and distress. The trials demonstrated statistically significant improvements on the primary endpoints, though the effect sizes were modest by conventional standards. Regulators approved the drug on the basis that even modest improvements carry meaningful quality-of-life significance for affected individuals.
That regulatory history matters to the research community for a specific reason: it established a documented safety and efficacy profile for one delivery route and one dose. The nasal delivery data from earlier trials, while informative, didn't reach the same evidentiary threshold. For researchers reviewing the full body of bremelanotide literature, that gap between the nasal phase and the approved subcutaneous formulation is worth understanding rather than glossing over.
One acknowledged limitation in the existing literature is that intranasal bremelanotide studies were conducted primarily in male populations with erectile dysfunction, while the approved indication targets premenopausal women with HSDD. The populations, endpoints, and delivery routes differ enough that drawing direct comparisons requires significant caution. Research examining this compound across both populations would benefit from more parallel-design studies using consistent outcome measures.
Outside clinical settings, PT-141 continues to appear in peptide research discussions as a nasal spray. Research-grade bremelanotide is available through peptide suppliers and is used by investigators, biohackers, and practitioners interested in the compound's profile. This use exists in a different context from the approved drug, and the two shouldn't be conflated.
Research-grade material is not subject to the same manufacturing controls as pharmaceutical-grade Vyleesi. Purity, sterility, and peptide concentration can vary between suppliers, which introduces additional variables that aren't present in approved clinical formulations. Anyone reviewing literature about nasal delivery research, or discussing research-grade use, should keep that distinction in mind.
Practitioners in the men's health and integrative medicine space have reported using compounded or research-grade intranasal bremelanotide, though the evidence base supporting this specific application remains limited compared to the approved subcutaneous route. According to practitioners working in this space, some individuals prefer the nasal route for convenience, despite the documented variability in absorption. That preference is understandable, but it's not evidence of equivalent efficacy or safety to the approved formulation.
Researchers comparing PT-141 to other compounds in the peptide space, including those examining BPC-157's tissue-level mechanisms or growth hormone secretagogues, often find bremelanotide interesting precisely because its mechanism is so distinct. It doesn't operate through repair pathways or GH axis stimulation. It targets a receptor system that bridges central nervous function and peripheral physiology in ways that remain incompletely understood.
Post-approval research on bremelanotide has expanded in several directions. Studies have examined its potential applications in male sexual dysfunction, particularly for men who don't respond adequately to PDE5 inhibitors. The central mechanism hypothesis makes it theoretically complementary to vasodilatory approaches, which has generated interest in combination research.
There's also ongoing investigation into MC4R agonism more broadly, including compounds with greater receptor selectivity and improved side-effect profiles. Setmelanotide, another melanocortin agonist with higher MC4R selectivity, has received approval for specific genetic obesity conditions, demonstrating that melanocortin pharmacology has applications well outside sexual health. That approval reinforced the importance of receptor subtype selectivity as a design consideration for future compounds.
The nasal delivery question hasn't been fully closed. Pharmaceutical researchers continue exploring intranasal delivery for centrally-acting peptides generally, partly because the nose-to-brain delivery hypothesis remains scientifically interesting even where it hasn't produced approved products. Better understanding of nasal mucosa permeability, absorption enhancers, and formulation technology may eventually make intranasal delivery of compounds like bremelanotide more reliable than early studies suggested.
For now, the honest summary of the evidence is this: intranasal PT-141 bremelanotide delivery has a legitimate research history, contributed meaningfully to understanding the compound's mechanism, and helped establish the case for eventual approval. The subcutaneous route became the approved path because it offered better pharmacokinetic consistency, not because the nasal approach was without merit.
This article is for informational and research purposes only. Nothing contained here constitutes medical advice, treatment recommendations, or encouragement to use any compound outside of supervised clinical or research settings. PT-141/bremelanotide is an FDA-approved prescription drug when used as Vyleesi, and research-grade materials exist in a separate regulatory context. Always consult a qualified healthcare provider before making decisions about any therapeutic compound. For research purposes only, not medical advice.