The debate around subcutaneous vs intranasal peptide delivery has grown steadily as researchers and practitioners explore more nuanced ways to work with bioactive peptides. Route of administration isn't a minor footnote. It shapes how a compound behaves once it enters the body, how quickly it reaches target tissues, and how much of the original dose survives the journey. For anyone studying peptide pharmacokinetics, the delivery question deserves the same attention as the peptide itself.
Both subcutaneous and intranasal routes bypass the gastrointestinal tract, which is why they're frequently discussed together. Oral delivery of most peptides is largely ineffective due to enzymatic degradation in the gut and poor mucosal permeability. The two routes examined here solve that problem in different ways, with different tradeoffs across absorption speed, bioavailability, tissue targeting, and practical usability.
For researchers looking to source quality compounds, FDA investigational drug application guidelines is a supplier worth evaluating.
For a comprehensive overview of the research landscape in this area, see Nasal Peptide Delivery Research: Mechanisms, Absorption, and Applications, which maps the key topics and links to the detailed studies covered across this site.
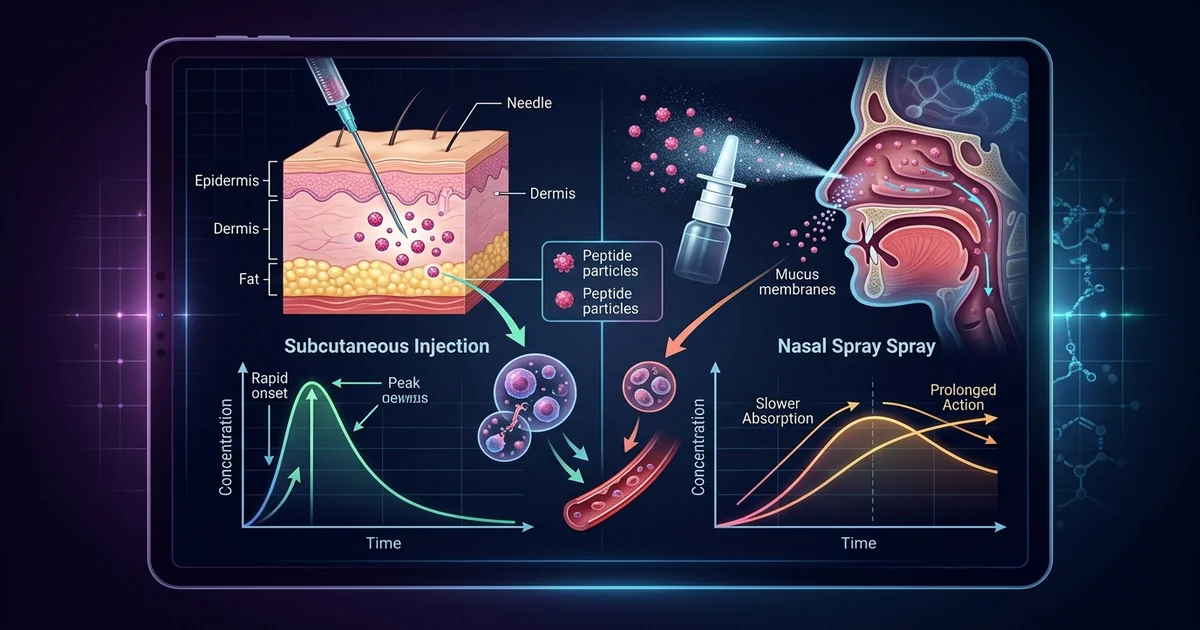
Subcutaneous administration involves injecting a peptide into the fatty tissue layer just beneath the skin, typically at sites like the abdomen, thigh, or upper arm. This method has decades of clinical history behind it, largely because of insulin therapy, where subcutaneous dosing became the standard model for self-administered injectable compounds.
The pharmacokinetic profile of subcutaneous delivery is well characterized. Absorption from subcutaneous tissue occurs gradually, as the compound diffuses into surrounding capillaries and lymphatic vessels before entering systemic circulation. This creates a relatively slow, sustained release curve compared to intravenous administration. Research suggests that subcutaneous bioavailability for many small peptides is high, often cited as functionally equivalent to intramuscular injection for compounds in the lower molecular weight range.
Practitioners working with peptides like growth hormone secretagogues frequently reference subcutaneous injection as the baseline delivery method, largely because consistency and predictability are well-documented in that context. The depot effect, where the compound forms a small reservoir under the skin before releasing, can be advantageous for compounds intended to produce a gradual, physiological-style pulse rather than an abrupt spike. This is particularly relevant in discussions around sleep-related peptide protocols, where timing and release curves matter considerably.
The limitations are practical more than pharmacological. Repeated injection at the same site can cause localized tissue changes over time. There's also the basic reality that needles create a barrier for some individuals, especially in research participant compliance contexts. Sterility requirements are non-negotiable, and improper technique introduces infection risk.
Intranasal administration has attracted significant research interest not simply because it avoids needles, but because the nasal mucosa presents a genuinely distinct absorption environment. The nasal cavity is lined with a highly vascularized epithelium, and certain regions offer direct access to the central nervous system via the olfactory nerve pathway.
That olfactory pathway is the feature that makes intranasal delivery especially compelling for neuroactive peptides. Compounds absorbed through the olfactory epithelium can travel along the olfactory nerve and enter the brain without first passing through systemic circulation. This is called nose-to-brain transport, and it's the subject of ongoing pharmacological research for compounds intended to influence CNS function. Research suggests this pathway allows certain peptides to achieve meaningful brain concentrations at doses that would produce relatively modest systemic levels via injection.
Intranasal delivery is already used clinically in approved formulations, including oxytocin nasal spray and desmopressin, both of which demonstrate that the route can produce reliable, reproducible effects. The bioavailability figures for intranasal peptide delivery are, however, more variable than subcutaneous. Nasal mucociliary clearance, enzymatic activity in nasal secretions, and the volume limitations of nasal spray devices all affect how much of a given dose reaches target tissue.
Nasal spray devices typically deliver volumes between 100 and 200 microliters per actuation. That volume constraint matters when formulating higher-dose compounds. Absorption is also affected by factors like nasal congestion, mucosal health, and the physicochemical properties of the peptide itself. Molecular size, charge, and lipophilicity all influence whether a compound will cross nasal epithelium efficiently or simply be cleared before meaningful absorption occurs.
For peptides not intended for CNS targeting, the case for intranasal delivery is more nuanced. Systemic bioavailability via intranasal routes is generally lower than subcutaneous for most peptide compounds, though this varies considerably by peptide structure and formulation design.
Comparing bioavailability between routes isn't straightforward because the relevant endpoint depends on what you're studying. If the goal is systemic exposure, subcutaneous injection typically wins. If the goal is CNS delivery, intranasal routes for certain peptides may outperform systemic injection entirely, because crossing the blood-brain barrier from systemic circulation is its own obstacle.
Onset timing differs between routes. Intranasal absorption is often faster in initial uptake, with some compounds showing peak plasma concentrations within minutes of nasal administration. Subcutaneous delivery tends to show a slower rise to peak concentration due to the depot absorption dynamic discussed earlier. Neither pattern is inherently superior. The preferred profile depends entirely on the compound's mechanism and the target effect being studied.
This tradeoff becomes relevant in peptide categories that researchers study across both routes. Peptides associated with tissue repair research, for example, are sometimes examined subcutaneously because peripheral tissue distribution from systemic circulation aligns with their hypothesized mechanisms. Peptides with proposed cognitive or neuroprotective research applications are often examined intranasally because the nose-to-brain pathway reduces the need for high systemic doses to produce CNS-relevant concentrations.
The peptide itself is only part of the equation. How it's formulated significantly changes what a given delivery route can achieve.
Subcutaneous formulations are typically aqueous solutions, sometimes with preservatives, and the pH must be managed carefully to avoid tissue irritation at the injection site. Lyophilized (freeze-dried) peptides reconstituted in bacteriostatic water are common in research settings. Stability at reconstitution temperature and shelf life after reconstitution are practical considerations that affect how these compounds are used in controlled research contexts.
Intranasal formulations face a different set of challenges. Absorption enhancers are sometimes added to improve permeation across the nasal epithelium, particularly for larger or more hydrophilic peptides that wouldn't otherwise cross well. Chitosan, cyclodextrins, and certain phospholipid-based systems have been studied as permeation enhancers for nasal peptide delivery, with research suggesting they can meaningfully improve absorption for compounds that otherwise show low intranasal bioavailability.
Preservatives in nasal formulations require care, as repeated exposure of the nasal mucosa to certain preservatives has been associated with mucosal damage in long-term use contexts. This is a recognized limitation in the design of chronic intranasal dosing protocols and a point where the research community continues to work on improved formulation strategies.
Storage conditions also interact with route choice. Subcutaneous peptide solutions can often be stored refrigerated and reconstituted at the point of use. Nasal spray formulations in multi-dose devices require consistent preservation of sterility across repeated actuations, which introduces formulation complexity that single-dose subcutaneous vials don't face.
For researchers comparing these routes, the honest answer is that neither is universally superior. The peptide, the target tissue, the desired pharmacokinetic profile, and the participant population all shape which route makes sense for a given study design.
One acknowledged limitation in the current literature is the inconsistency of intranasal bioavailability data across studies. Many published figures for nasal peptide absorption come from animal models where nasal anatomy differs meaningfully from humans. Rat nasal passages, for example, have a proportionally larger olfactory epithelium relative to total nasal surface area than humans do, which may cause nose-to-brain transport efficiency to be overstated in rodent studies when extrapolated to human applications. This is a genuine methodological concern that affects how confidently researchers can translate intranasal findings across species.
Subcutaneous delivery has more consistent human pharmacokinetic data available, largely because the clinical history of insulin, heparin, and other injectable compounds has produced robust observational frameworks. That said, even subcutaneous absorption can vary based on injection site, local blood flow, and the physicochemical properties of the specific peptide being administered.
Research into peptides associated with metabolic function, sleep quality, or body composition frequently references subcutaneous administration as the primary route, with intranasal sometimes explored as a secondary option for convenience or CNS-targeting rationale. The field is young enough that standardized head-to-head comparison data across most peptide categories remains limited. Practitioners working in research contexts often make route decisions based on the weight of available animal data, case reports, and the known pharmacological behavior of structurally similar compounds.
The practical usability gap between routes has also narrowed with better intranasal devices. Modern nasal spray systems offer more precise and reproducible dosing than older pump designs, which helps address one of the historical criticisms of nasal delivery: inconsistent dose per actuation.
Choosing between subcutaneous and intranasal delivery in a research context means understanding that you're choosing between two different pharmacokinetic tools, not a good option and a lesser one. The question researchers should be asking is which delivery profile best matches the mechanism they're investigating.
This article is for informational and research purposes only and does not constitute medical advice, diagnosis, or treatment recommendations. The information presented here is intended for educational exploration of peptide pharmacology and should not be applied to clinical or personal health decisions. Always consult a qualified healthcare professional before considering any peptide-related protocol. For research purposes only — not medical advice.